Your Gut Is Driving Your Chronic Pain. Here Are Eight Reasons Why Nobody Connected The Dots.
- Jason Winkelmann
- 4 hours ago
- 12 min read

TL;DR
Most chronic pain patients have gut symptoms. Most chronic pain specialists send them to a gastroenterologist. Most gastroenterologists do not connect what they find back to the pain. The result is that one of the most significant and most treatable contributors to chronic pain goes completely unaddressed, often for years. Intestinal permeability, food sensitivities, gut dysbiosis, short-chain fatty acid deficiency, vagus nerve dysregulation, neurotransmitter depletion, tryptophan pathway disruption, and the gut-opioid connection are eight distinct mechanisms through which your gut health is actively producing and sustaining your chronic pain. This article covers all eight.
What Most Patients Are Told
If you have chronic pain and you also have gut symptoms, the typical response from the medical system is to treat them as two separate problems.
Your pain specialist manages your pain. Your primary care doctor refers you to a gastroenterologist. The gastroenterologist evaluates your gut. And somewhere in the middle of that referral chain, the connection between what is happening in your intestinal tract and what is happening in your nervous system gets lost entirely.
This is not a minor gap. It is one of the most consequential oversights in chronic pain management, and it is happening to almost every chronic pain patient in the conventional medical system.
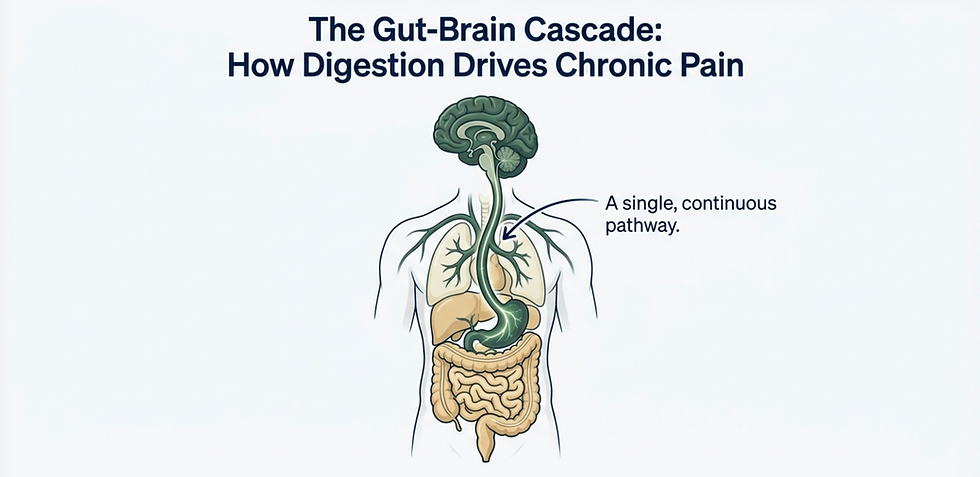
What you are almost never told is that your gut is not just a digestive organ. It is an immune organ, a neurotransmitter production facility, a hormonal regulator, and a direct communicator with the pain-processing centers of your brain. When it is functioning poorly, all of those systems are affected, and every one of them has a direct, documented pathway to chronic pain.
Where The Conventional Explanation Breaks Down
Chronic pain treatment that focuses only on the nervous system, the muscles, or the joints is working with an incomplete model. The gut is not a peripheral variable in chronic pain. It is a central one.
The eight mechanisms covered in this article are not theoretical connections. They are specific, documented pathways through which gut dysfunction produces inflammation, activates immune cells, disrupts neurotransmitter balance, opens the pain gate in your spinal cord, and renders pain medications progressively less effective.
Treating any of them in isolation, or treating none of them because the connection was never made, is one of the primary reasons so many chronic pain patients cycle through treatments without achieving meaningful recovery.
Mechanism One: Your Gut Lining Is One Cell Thick, And When It Breaks, Everything Downstream Changes
The lining of your small intestine is a single cell layer thick. Those cells, called enterocytes, are packed tightly together and held in place by structures called tight junctions. Under normal conditions, food particles travel through the intestinal tract, get broken down, and pass through individual enterocytes before entering the bloodstream in a controlled, fully-digested form.
Intestinal permeability, often called leaky gut, occurs when those tight junctions break apart. The cells begin to separate. Food particles that have not been fully digested slip between the cells and enter the bloodstream directly.

Your immune system encounters those particles and does what it was designed to do: it treats them as foreign invaders and produces inflammation to signal the rest of the body that something is wrong. In the context of a one-time event, this is an appropriate response. In the context of every meal, every day, it becomes a source of chronic systemic inflammation.
Chronic inflammation is not the visible, localized kind you see when you sprain an ankle. It does not announce itself. It builds silently in the background over time, and it is a hallmark of virtually every chronic pain condition. As long as intestinal permeability is present and unaddressed, the immune system remains chronically activated, chronic inflammation continues to accumulate, and the pain system has a sustained biochemical input keeping it sensitized.
This is also why chronic pain and autoimmune conditions so frequently occur together. A chronically activated immune system, driven by repeated exposure to undigested food particles crossing a damaged gut barrier, is the shared mechanism.
Mechanism Two: Food Sensitivities Are Not Allergies, And The Distinction Changes Everything About Testing
When most people hear food sensitivity, they think food allergy. These are not the same thing, and the difference matters enormously for testing and treatment.
Your immune system produces several classes of proteins called immunoglobulins: IgA, IgG, IgM, and IgE. A true food allergy is an IgE reaction. It is immediate and unmistakable. You eat a peanut, your throat swells, you get hives. The body responds within minutes and the trigger is obvious.
A food sensitivity is an IgG or IgA reaction. It is delayed, sometimes by hours, sometimes by days. The symptom that follows may bear no obvious relationship to the food that triggered it. Pain flares, fatigue, brain fog, and inflammation spikes in the hours or days after consuming a food that the immune system is reacting to. Without testing, the connection is almost impossible to identify on your own.

When the immune system reacts to a food through the IgG or IgA pathway, the first thing it does is produce inflammation. Continued consumption of that food means continued immune activation, continued inflammation, and, critically, downregulation of both opioid and NMDA receptors, making the nervous system more sensitive to pain and making pain medications less effective simultaneously.
The same eight foods account for approximately ninety percent of food sensitivities: dairy, eggs, peanuts, tree nuts, wheat, soy, fish, and shellfish. But unusual sensitivities to foods like chicken or watermelon are possible and go undetected without proper testing.
Testing is where most people run into problems. Standard allergy testing from an allergist measures IgE reactions only. At-home test kits have poor sensitivity and specificity, producing results that are not reproducible from one test of the same sample to the next. The appropriate test is a CLIA-certified food sensitivity panel through a clinical provider that measures both IgG and IgA reactions, because it is possible to have an IgA reaction without an IgG reaction or vice versa, and missing one can mean missing a significant contributor to chronic pain.
One more important note. When a food sensitivity panel comes back with a large number of flagged foods, that is almost never a sign that all of those foods need to be permanently eliminated. It is typically a sign that intestinal permeability is present and generating widespread immune reactivity. Fix the gut lining, and the majority of those sensitivities resolve on their own.
Mechanism Three: The Bacteria in Your Gut Are Producing Inflammation That Reaches Your Brain
Your gut microbiome is the collection of bacteria living in your intestinal tract. Those bacteria are broadly divided into two categories: bacteroidetes, which are generally beneficial, and firmicutes, which are generally harmful in excess. When the balance between them is maintained, the system functions well. When firmicutes begin to dominate, which happens with poor diet, antibiotic use, stress, and chronic pain itself, a cascade of consequences follows.
The most immediately relevant of these is the release of a compound called lipopolysaccharide, or LPS, an endotoxin produced by harmful bacteria. LPS on its own is damaging. LPS in the presence of intestinal permeability, where it can cross the gut barrier directly into circulation, is significantly more so. And LPS makes intestinal permeability worse, creating a cycle that compounds itself.
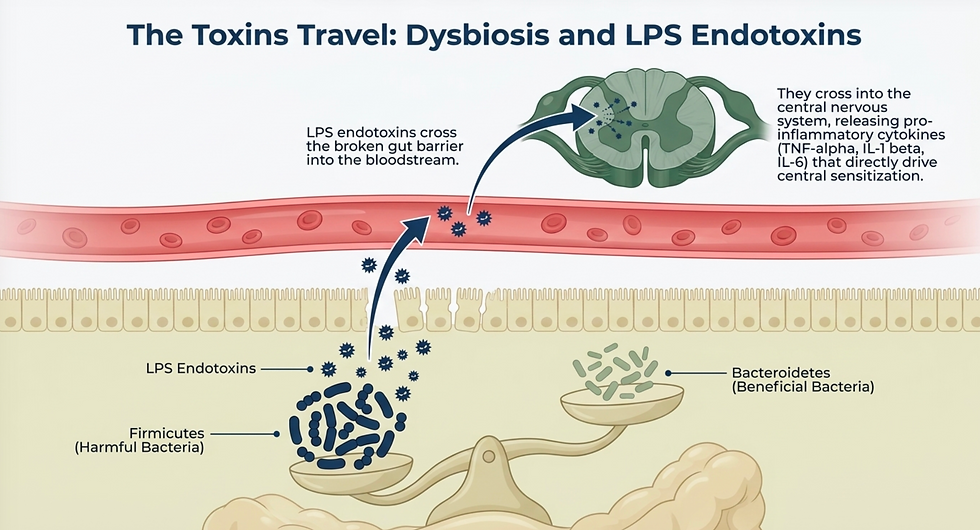
When LPS enters the bloodstream, it triggers the production of pro-inflammatory cytokines including tumor necrosis factor alpha, interleukin-1 beta, and interleukin-6. These cytokines do not stay in the periphery. They cross into the central nervous system, where they sensitize pain-processing pathways in the brain and spinal cord and directly contribute to the central sensitization that drives widespread, persistent chronic pain.
This is why chronic pain patients frequently experience pain that is far removed from any identifiable site of injury. The generator is not in the joint, the muscle, or the nerve. It is in the gut, and it is reaching the central nervous system through the bloodstream.
Mechanism Four: You Are Probably Not Getting Enough Fiber, And Your Nervous System Is Paying The Price
When the balance of beneficial bacteria in the gut is healthy and dietary fiber intake is adequate, beneficial bacteria ferment that fiber and produce compounds called short-chain fatty acids: specifically butyrate, acetate, and propionate.
These are not minor metabolic byproducts. They are some of the most therapeutically important compounds in the body, and most chronic pain sufferers are significantly deficient in all three.
Butyrate is the primary fuel source for the cells lining the large intestine. It also upregulates the tight junction proteins that hold the gut lining together, directly reducing intestinal permeability and addressing the root of the first mechanism in this article. Acetate travels to the liver and supports detoxification, reducing the inflammatory and free radical burden from environmental toxins. Propionate also reaches the liver and assists with glucose metabolism, reducing the chronic inflammation and advanced glycation end product accumulation that come from blood sugar dysregulation.

Collectively, short-chain fatty acids reduce chronic inflammation, improve immune function, decrease food sensitivity reactivity, improve insulin sensitivity, and increase mineral absorption including magnesium, one of the most critical nutrients for pain modulation.
The path to adequate short-chain fatty acid production runs directly through gut microbiome health and dietary fiber intake, neither of which is typically evaluated or addressed in standard chronic pain care.
Mechanism Five: Your Vagus Nerve Is Delivering Danger Signals from Your Gut to Your Brain's Pain Centers
The vagus nerve is the primary communication channel between the gut and the brain. It is a parasympathetic nerve, meaning it belongs to the branch of the autonomic nervous system associated with rest, digestion, and recovery.
Eighty percent of the vagus nerve's activity is afferent, meaning it carries signals from the body up to the brain rather than the other way around. Under healthy conditions, those signals support calm, restorative nervous system function.

When the gut is producing LPS, chronic inflammation, and microbial imbalance, the vagus nerve picks up those signals and delivers them to a region of the midbrain called the periaqueductal gray. This structure is one of the most important pain-modulation centers in the entire nervous system. It is responsible for threat processing, survival behaviors, and critically, descending inhibition: the mechanism by which the spinal cord filters incoming signals and prevents insignificant inputs from reaching the brain as pain.
When the periaqueductal gray is activated by danger signals traveling up the vagus nerve from a dysregulated gut, descending inhibition weakens. The gate opens. Signals that should be filtered out are allowed through. Pain is experienced to things that should not cause pain, and existing pain is amplified beyond what the underlying tissue damage would justify.
This is the same mechanism by which emotions, fear, anxiety, and catastrophizing thoughts drive chronic pain. The vagus nerve, the periaqueductal gray, and the descending inhibition pathway are the shared anatomical pathway between gut health and emotional health, and both are actively contributing to your pain through the same gate.
Mechanism Six: Ninety Percent of Your Serotonin Is Made in Your Gut, and Your Pain System Depends on It
Serotonin is most commonly discussed in the context of mood. What almost no one explains is that approximately ninety percent of the body's serotonin is produced not in the brain but in the gut, by specialized cells regulated by the gut microbiome.
Serotonin is a critical input to the descending inhibition system. It is one of the primary neurotransmitters used by the inhibitory interneurons in the spinal cord to keep pain signals from reaching the brain inappropriately. When serotonin production falls, that inhibitory capacity falls with it, and the pain gate weakens.

Gut bacteria are also directly involved in the production of GABA, dopamine, and norepinephrine, all of which contribute to pain modulation and descending inhibition. When the microbiome is dysregulated, the production of every one of these neurotransmitters is affected, and the chronic pain sufferer loses multiple layers of the nervous system's own pain-management capacity simultaneously.
This is the physiological basis for why addressing gut health produces neurological improvements that go far beyond digestive symptoms. The gut is not adjacent to the neurotransmitter system. It is a primary production facility for it.
Mechanism Seven: Your Gut Is Hijacking the Pathway That Should Be Making Serotonin
Under normal conditions, the amino acid tryptophan, obtained from dietary protein, is converted into serotonin. When gut dysbiosis is present, that conversion pathway is disrupted.
Instead of traveling the serotonin pathway, tryptophan gets redirected into what is called the kynurenine pathway, which produces a compound called quinolinic acid. Quinolinic acid is a potent activator of the NMDA receptor, the same receptor that sits at the center of central sensitization. When the NMDA receptor is activated by quinolinic acid, the gate in the spinal cord opens, more pain signals reach the brain, and central sensitization intensifies.
Magnesium and vitamin B6 both help reduce quinolinic acid levels, but targeting them in isolation is addressing the wrong end of the problem. The quinolinic acid is being produced because the gut dysbiosis redirected tryptophan away from serotonin synthesis in the first place. That is where the intervention needs to begin.
This single mechanism connects gut microbiome health directly to the NMDA receptor, to central sensitization, and to the neurotransmitter deficit that weakens descending inhibition. It is one of the clearest illustrations of why treating chronic pain without treating the gut is treating the consequence without the cause.
Mechanism Eight: Your Opioids Are Working Less Well Because of What They Are Doing to Your Gut
This is one of the most important and least discussed connections in chronic pain management.
Opioids reliably slow bowel motility. This is so well known it is almost treated as a minor inconvenience. It is not. Slowed bowel movement creates the conditions for gut dysbiosis: more harmful bacteria, less beneficial bacteria, and a significant reduction in short-chain fatty acid production. Less butyrate means the tight junctions in the gut lining are no longer being maintained. Intestinal permeability develops or worsens. LPS from harmful bacteria begins crossing into circulation.

That LPS triggers pro-inflammatory cytokine production. That inflammation travels to the nervous system, where it does two things that directly undermine the medication that caused the gut problem in the first place: it desensitizes opioid receptors, making the drug less effective at the receptor level, and it reduces the number of opioid receptors expressed on the nerves.
The inflammation also activates the NMDA receptor, opening the pain gate and amplifying central sensitization. Glutamate production increases. GABA production decreases. The result is a nervous system that is more sensitized, a gut that is more compromised, and an opioid that requires progressively higher doses to produce the same effect because the receptor it is targeting is being degraded by the very biological cascade the medication initiated.
If opioids are part of your current treatment plan and you want to make them safer and more effective, the gut is where that work begins.
The Bottom Line
Your gut and your chronic pain are not two separate problems being managed by two separate specialists.
They are the same problem, expressed through eight overlapping biological pathways that all feed the same outcome: a chronically sensitized nervous system, a depleted neurotransmitter supply, a weakened descending inhibition system, and a pain cycle that no amount of peripheral intervention will fully interrupt.
A chronic pain treatment plan that does not evaluate and address gut health is working with less than half the picture, and the half it is missing is often the most important one.
If your chronic pain specialist has never asked about your gut, that is not a gap in your history. It is a gap in your care.

Written By:
Dr. Jason Winkelmann
Naturopathic doctor, Chiropractor, Chronic Pain Specialist, and Educator
Frequently Asked Questions
Do I need to have gut symptoms to have gut-driven chronic pain?
No, and this is one of the most important points in this entire article. Many of the mechanisms described, particularly LPS translocation from gut dysbiosis and the downstream effects on the NMDA receptor and neurotransmitter production, produce systemic effects without producing obvious digestive symptoms. You can have significant intestinal permeability and gut microbiome dysbiosis and experience no bloating, no reflux, and no bowel irregularity that would prompt you to think your gut is involved. The absence of gut symptoms does not rule out the gut as a driver of your chronic pain. It simply means the symptoms are expressing elsewhere.
What is the difference between a food sensitivity test and an allergy test, and why does it matter for chronic pain?
Standard allergy testing measures IgE reactions, which are immediate and anaphylactic in nature. Food sensitivities involve IgG and IgA immune responses that are delayed by hours or days and produce inflammation rather than anaphylaxis. For chronic pain purposes, IgE testing is almost entirely irrelevant. What matters is the IgG and IgA response that is generating chronic immune activation and inflammation. The appropriate test is a CLIA-certified food sensitivity panel through a clinical provider that measures both IgG and IgA, not an at-home kit, and not a standard allergy panel from an allergist.
If my food sensitivity panel comes back with many flagged foods, does that mean I need to eliminate all of them?
In most cases, no. When a large number of foods are flagged on a sensitivity panel, the most likely explanation is that intestinal permeability is present and is causing widespread immune reactivity to foods that are crossing the gut barrier in an undigested state. The reactive foods are a symptom of the permeability, not independent problems requiring permanent elimination. Addressing the gut lining, the microbiome balance, and short-chain fatty acid production typically resolves the majority of those sensitivities over time without requiring lifetime food avoidance.
How does gut dysbiosis affect my pain medications specifically?
Gut dysbiosis reduces short-chain fatty acid production, which impairs gut barrier integrity, which allows LPS from harmful bacteria to enter circulation, which triggers pro-inflammatory cytokine production, which desensitizes opioid receptors and reduces their expression on nerve cells. Simultaneously, the resulting neuroinflammation activates the NMDA receptor, increases glutamate production, decreases GABA production, and opens the pain gate in the spinal cord. The medication is working against a biological environment that is actively degrading the receptor it depends on. This is the mechanism behind opioid tolerance, and it is directly addressable through gut health interventions.
Where should someone start if they want to address the gut component of their chronic pain?
The starting point is evaluation, because the appropriate interventions depend on what is actually present. Intestinal permeability, food sensitivities, microbiome dysbiosis, and short-chain fatty acid deficiency are related but distinct findings that require different primary interventions. Working with a provider who understands both the gut mechanisms and their connection to the pain system, who can run appropriate testing including CLIA-certified food sensitivity panels and comprehensive stool analysis, and who can build a treatment plan that addresses gut health as a core component of chronic pain care rather than a separate referral is the most effective starting point.



Comments