How Chronic Pain Treatments Work: Triptans, Nerve Blocks, Stellate Ganglion Blocks, and Muscle Relaxers
- Jason Winkelmann
- 3 minutes ago
- 13 min read


TL;DR
Triptans, nerve blocks, stellate ganglion blocks, and muscle relaxers are among the most commonly used interventions for migraine and musculoskeletal chronic pain. Each one works through a mechanism that is far more specific and far more consequential than most patients are ever told. Understanding how each of these works inside the body, why the side effects happen, and what the underlying biology actually needs instead is not a minor detail. It is the difference between managing a condition indefinitely and having a genuine path toward resolving it.
What Most Patients Are Told
If you live with migraines, you have probably been handed a triptan and told it will stop the attack. If your pain is localized and severe, a nerve block may have been recommended. If your muscles are chronically tight, a muscle relaxer has likely been part of the conversation.
What almost never accompanies these prescriptions is a clear explanation of what they are doing at the level of the tissue, the nerve, or the nervous system; and more importantly, what they are not doing.
Most people in chronic pain have a sense that their medications treat symptoms without fixing anything. What they rarely have is the specific physiological vocabulary to understand why that is true, why certain side effects are inevitable given the mechanism, and what a more complete approach would actually look like.
That is what this article covers.
Where The Conventional Explanation Breaks Down
Each medication in this article targets a real mechanism. Triptans are pharmacologically sophisticated. Nerve blocks are clinically useful. Muscle relaxers address a genuine physiological problem. None of this is in dispute.
What each medication shares is a boundary. A point at which the intervention stops and the underlying condition continues. For acute, self-resolving problems, that boundary rarely matters. For chronic pain, it is the central issue.
Understanding exactly where each medication's reach ends is the first step toward understanding what a treatment plan needs to include beyond it.
Triptans: Three Mechanisms, Two Significant Gaps
Triptans are among the more mechanistically complex medications used in migraine management. They work through three simultaneous pathways. Each one is worth understanding in its own right, because together they tell you a great deal about what is actually driving your migraines.

Three Things Triptans Do Inside Your Body
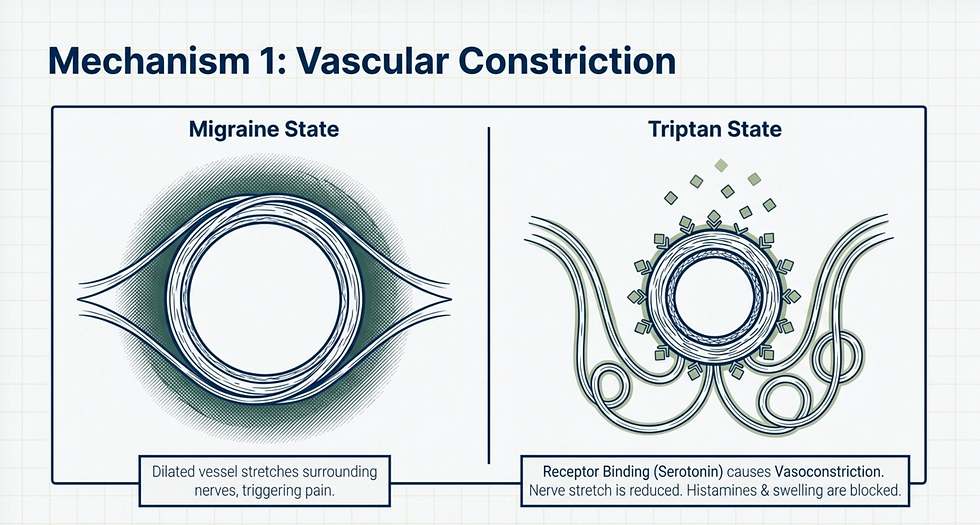
First, triptans bind to serotonin receptors on blood vessels, causing them to constrict. During a migraine, blood vessels in the head dilate, and that dilation stretches the pain-sensing nerves that run alongside them. Vasoconstriction reduces that stretch, and it does something else as well: it reduces the flow of histamines and pro-inflammatory prostaglandins reaching the brain, reduces the throbbing pulsation associated with vascular dilation, and limits the swelling that eventually reaches the meninges (the membrane surrounding the brain, which is heavily supplied with pain-sensing nerve fibers).
Second, triptans block the release of CGRP (calcitonin gene-related peptide) the potent vasodilator at the center of the migraine cascade. When CGRP release is blocked, a secondary effect follows: substance P, a neuropeptide released by damaged tissues to generate pain and inflammation, is also reduced. Blocking one suppresses the other.

Third, triptans influence descending inhibition — the spinal cord's mechanism for regulating how much of any pain signal actually reaches the brain. Under normal conditions, inhibitory interneurons release serotonin and norepinephrine between nerve junctions to block excessive pain transmission. Triptans bind to serotonin receptors on the first nerve in the chain, effectively doing the job those inhibitory interneurons should be doing: preventing excitatory neurotransmitters like CGRP and glutamate from jumping to the next nerve and continuing toward the brain.

This is a genuinely impressive set of mechanisms. But it has two gaps that matter significantly.
What Triptans Assume About Your Migraine
The entire mechanism depends on one assumption: that your migraine is being driven by trigeminal nerve activation, CGRP release, and subsequent blood vessel dilation. If your migraine has a different primary driver, triptans will not work for you. And the fact that they do not work for a meaningful percentage of migraine sufferers is the clearest evidence that the CGRP-vasodilation pathway is not the only one involved.
If triptans work for you, that information is actually useful. It tells you something specific about the pathway driving your migraines. If they do not, that is equally useful. It tells you the search needs to go elsewhere.
Why Triptans Affect Far More Than Your Head
The serotonin receptors that triptans target are found on blood vessels throughout the entire body, not just in your head. When a triptan is taken, vasoconstriction occurs systemically. This is why side effects include chest tightness, pressure sensations, flushing, tingling, dizziness, and fatigue. These are not incidental effects. They are the direct consequence of constricting blood vessels that were never the target of treatment.
In most patients without underlying cardiovascular conditions, these effects are mild and tolerable. In anyone with pre-existing cardiovascular disease, arterial disease, or a history of stroke, triptans are contraindicated for precisely this reason. Systemic vasoconstriction in a compromised vascular system carries real risk.
The Natural Alternative: Support the Biology That Triptans Are Compensating For
If triptans work for your migraines, they are telling you which biological systems are underperforming. The medications are compensating for insufficient serotonin, excessive CGRP activity, and inadequate descending inhibition. The more useful long-term target is restoring those systems rather than substituting for them.
Increasing serotonin starts with the amino acid tryptophan, meaning adequate protein intake is foundational. The conversion of tryptophan into serotonin requires specific cofactors: iron, magnesium, calcium, vitamins B6, B9, and C, and zinc. Without adequate levels of these, the pathway stalls regardless of how much tryptophan is available.
Reducing CGRP activity has natural support as well. Magnesium, CoQ10, curcumin, and the herb butterbur all have documented CGRP-inhibiting activity. They are not as pharmacologically potent as triptans or dedicated CGRP inhibitor medications, but as part of a treatment approach that is also addressing the triggers and the underlying system instability, they contribute meaningfully.
Blocking glutamate at the receptor — one of the key excitatory neurotransmitters driving nerve transmission during a migraine — is another documented function of magnesium, which continues to be one of the most therapeutically versatile compounds in migraine management.
Nerve Blocks: Valuable Diagnostics With Physiological Limits
How Nerve Blocks Actually Work
To understand nerve blocks, you need to understand how a nerve fires and resets.
At rest, a nerve is in a balanced electrical state. When a stimulus arrives, sodium rushes into the nerve through specialized channels, generating a charge that moves down the length of the nerve toward the brain — carrying the pain signal with it. Once that signal has passed, potassium inside the nerve rushes out to reset the electrical balance.

A nerve block works by injecting a local anesthetic (lidocaine, bupivacaine, or ropivacaine) that binds to and blocks those sodium and potassium channels. The nerve can receive a stimulus, but it cannot generate or sustain a signal. It also cannot reset and fire again. The pain signal stops.

Their Diagnostic Value — Which Is Often More Important Than The Relief Itself
This is a point that deserves more emphasis than it typically receives.
Chronic pain is frequently generated somewhere other than where it is felt. The location of your pain and the location of its source are often not the same. And that disconnect makes diagnosis genuinely difficult. Nerve blocks offer something that most other treatments do not: a clear test of whether a specific nerve is involved in generating or transmitting your pain.
If a block of a particular nerve produces meaningful relief, that is direct evidence that the nerve is part of the pathway. Treatment can then be focused there with confidence. If the block produces no change, that is equally valuable. It eliminates that nerve from the conversation and points elsewhere. This kind of diagnostic clarity is rare in chronic pain management and should not be undervalued.
Why There Is No Natural Equivalent — And Why That Is Fine
Sodium and potassium channel blockade at the level of a specific nerve has no natural equivalent, and there is no supplement or dietary intervention that replicates it. But that is not a problem, because replicating it is not the right goal.
Pain is a symptom. It is your nervous system telling you that something is wrong. It is not the thing that is wrong. A nerve block silences the messenger — which is sometimes exactly what is needed diagnostically, and occasionally what is needed therapeutically in an acute situation. But the underlying inflammation, the mechanical dysfunction, the metabolic disruption, or the central sensitization that is causing that nerve to fire has not been addressed.
Nerves do not fire without an input. Every nerve block wears off. If the input is still present when it does, the pain returns because nothing that was driving the symptom has changed.
The appropriate response to that reality is not a better nerve block. It is identifying and treating the input.
Stellate Ganglion Blocks: When the Target Is Your Nervous System Itself
What the Stellate Ganglion Actually Does
Most nerve blocks target a peripheral nerve, a specific pathway carrying a specific signal. A stellate ganglion block is different in a way that is worth understanding clearly.
The stellate ganglion is a collection of nerve cell bodies located at the junction of the neck and upper thoracic spine. It functions as a major relay station for the sympathetic nervous system — your fight-or-flight branch — distributing sympathetic outflow to the head, neck, upper extremities, and heart.

Injecting a local anesthetic into or near the stellate ganglion temporarily interrupts that sympathetic outflow across a wide area. The effect goes far beyond what a localized nerve block can produce.
Why Sympathetic Dominance Is Central to Chronic Pain
This is one of the most under-recognized mechanisms in chronic pain, and it is worth dwelling on.
Most chronic pain sufferers are living in a state of persistent sympathetic dominance. The autonomic nervous system has two branches — sympathetic, which prepares the body for threat, and parasympathetic, which supports rest, digestion, and recovery. These two are meant to balance each other. In chronic pain, driven by persistent perceived threat, the sympathetic branch dominates, and the parasympathetic branch rarely gets the opportunity to do its job.
In that state, adrenaline output is elevated. Heart rate is elevated. Muscle tension is elevated. And pain sensitivity is elevated. The nervous system is primed to detect and amplify threat signals because that is what a threat environment requires.
A stellate ganglion block temporarily quiets that sympathetic dominance in a way that is difficult to achieve through any other rapid intervention. For conditions where sympathetic overdrive is a central driver (complex regional pain syndrome and PTSD-related pain conditions in particular), the block can produce a meaningful reset that allows other treatments to be more effective.
The side effects reflect exactly what the sympathetic nervous system controls. Hoarseness, drooping of one eyelid, facial warmth, altered sweating patterns, and dizziness all occur because the stellate ganglion coordinates sympathetic signaling to structures that manage blood vessel tone, pupil response, sweating, and facial function. When that outflow is interrupted, those functions are temporarily altered.
The Natural Alternative: Restore Autonomic Balance
The goal is never to eliminate sympathetic activity. It is to restore the balance between sympathetic and parasympathetic function so that the body can move fluidly between states of appropriate alertness and genuine recovery.
In clinical practice, constitutional hydrotherapy is one of the most effective tools for retraining autonomic nervous system balance. The alternating thermal and electrical stimuli challenges the vasodilatory and vasoconstrictive response systems in a way that progressively improves their coordination and reduces sympathetic dominance over time.
Outside the clinical setting, the interventions that have the most consistent research support are meditation, yoga, tai chi, and structured breathwork. This is acknowledged in the research not because these are comfortable suggestions, but because the evidence base behind them for autonomic regulation is conclusive. They work. The barrier is not availability — it is consistency.
Muscle Relaxers: Two Types, Two Mechanisms, One Shared Limitation
Muscle relaxers are not a single category of drug. They work through two completely different mechanisms, and understanding the distinction matters for understanding both their effects and their limitations.
Centrally Acting Muscle Relaxers
Medications like cyclobenzaprine, tizanidine, and baclofen work in the central nervous system: specifically by modulating serotonin, glutamate, and GABA receptors in the brain and spinal cord.

To understand what they are correcting, it helps to understand what muscle tone actually means. Muscle tone is not about how defined or developed a muscle looks. It refers to the baseline level of partial contraction that muscles maintain at rest. This is normal and necessary. Without some resting tone, muscles cannot respond quickly when asked to move.
The problem arises when the brain is chronically sensing threat. Under sympathetic dominance, the brain increases baseline muscle tone so the body is more ready to fight or flee at any moment. For someone living with chronic pain, where the perceived threat never resolves, that elevated tone becomes the persistent baseline. The muscles are always partially braced, always using more energy than they should, always restricting blood flow to some degree.
Centrally acting muscle relaxers bring that tone back toward an appropriate resting level by working on the neurotransmitter systems that regulate it. Because they target specific receptor types rather than broadly suppressing muscle function, they generally do not interfere with normal voluntary muscle activity.
Peripherally Acting Muscle Relaxers
Peripherally acting muscle relaxers do not work on the central nervous system at all. They work directly on the muscles themselves, at a receptor called calmodulin.
Calmodulin is the switch that initiates muscle contraction. When calcium binds to it, the muscle fibers are pulled together and the muscle contracts. As long as calcium remains bound to calmodulin, the muscle stays contracted. The only way to release that contraction is to displace the calcium, and the molecule that does this is magnesium.

Peripherally acting muscle relaxers work by occupying the calmodulin receptor so that calcium cannot bind as readily. Less calcium binding means less contraction. The problem is that this mechanism is not selective. Every muscle in the body has calmodulin. The relaxer affects all of them, not just the ones that are pathologically tight. The result is reduced coordination, impaired muscle function, and the general sense of heaviness or weakness that many patients report with these medications.
Why Muscle Tone Is a Nervous System Problem, Not Just a Muscle Problem
This is the limitation both categories share, expressed at different levels.
Centrally acting relaxers address the nervous system output that is driving elevated tone, but they do not resolve what is keeping the nervous system in a threat state in the first place. Peripherally acting relaxers address the muscle-level mechanism, but entirely bypass the nervous system signal that is causing the muscle to remain contracted.
In both cases, when the medication is reduced or discontinued, the elevated tone returns. The autonomic state, the inflammatory environment, or the mechanical inputs that drove the elevation have not changed.
The Natural Alternatives
Magnesium is the most direct natural equivalent to a peripherally acting muscle relaxer. It competes with calcium for the calmodulin receptor. The difference from a pharmaceutical peripheral relaxer is that magnesium is the molecule the body was designed to use for this purpose, operating through the same mechanism rather than artificially blocking the receptor.
Improving blood flow to the muscle is equally important. A muscle that is not receiving adequate oxygen and ATP cannot complete the relaxation cycle regardless of how much magnesium is present. Relaxation is actually more energetically demanding than contraction — a fact that surprises most people — and a muscle that is chronically depleted of oxygen and mitochondrial energy will stay contracted not because it is receiving a signal to do so, but because it lacks the resources to do otherwise. This is fundamentally a mitochondrial function problem, and treating it requires treating the metabolic environment of the tissue.

Addressing the autonomic nervous system is the element that determines whether any of the above is sufficient. If the brain remains in a persistent state of threat detection, it will override all of it — continuing to drive elevated muscle tone regardless of what is happening at the level of the receptor or the tissue. Constitutional hydrotherapy, meditation, yoga, tai chi, and breathwork are not soft suggestions appended to the real treatment. They are the treatment for the input that keeps resetting the problem.

The Pattern That Runs Through All of It
Triptans compensate for insufficient serotonin, excessive CGRP, and inadequate descending inhibition — without restoring any of those systems.
Nerve blocks interrupt the pain signal — without addressing what is generating it.
Stellate ganglion blocks temporarily quiet sympathetic overdrive — without resolving the chronic threat state that sustains it.
Muscle relaxers reduce elevated muscle tone — without treating the nervous system, the inflammatory environment, or the metabolic depletion that produced and maintains it.
In every case, the medication is downstream of the actual problem. It is managing a consequence while the cause continues. In acute situations, that is often appropriate. In chronic pain, it is the central reason why the pain remains chronic.
The Bottom Line
Every medication in this article does something real. The physiology is sound and the mechanisms are well understood.
What none of them do is change the conditions that made the body generate the pain in the first place. And in chronic pain, that is the only thing that actually matters.
Managing a signal your body is generating for a reason is not the same as giving your body what it needs to stop generating it.

Written By:
Dr. Jason Winkelmann
Naturopathic doctor, Chiropractor, Chronic Pain Specialist, and Educator
Frequently Asked Questions
My triptans used to work and now they don't. Why does that happen?
Triptans work when your migraine is being primarily driven by trigeminal activation, CGRP release, and vasodilation. Over time, as central sensitization progresses — meaning the nervous system becomes more globally sensitized to pain — the central component of the migraine becomes increasingly dominant relative to the vascular component. Triptans address the vascular mechanism well. They address central sensitization poorly. As the balance between the two shifts, the medication loses the portion of its effect that was providing relief.
If a nerve block only provides temporary relief, is it worth doing?
Often, yes — specifically for its diagnostic value. If you receive a block to a particular nerve and your pain resolves significantly, you now have direct evidence that nerve is involved in generating or transmitting your pain. That information focuses your treatment in a way that might otherwise take much longer to establish. Temporary relief paired with diagnostic clarity is a meaningful outcome even when the block is not a long-term solution.
Is a stellate ganglion block appropriate for most chronic pain patients?
It is most clearly indicated when sympathetic nervous system overdrive is a central driver of the pain — as in complex regional pain syndrome and PTSD-related pain conditions. For other chronic pain presentations, the autonomic nervous system component may be significant but not the primary driver, in which case less invasive approaches to autonomic regulation are appropriate first-line interventions. It is worth a specific conversation with a provider who understands the role of the autonomic nervous system in your particular pain presentation.
Why does it take more energy to relax a muscle than to contract one?
Contraction is driven by the calcium-calmodulin interaction, which requires relatively little active energy expenditure. Relaxation requires actively pumping calcium back out of the cell and replacing it with magnesium — a process that depends on ATP-powered ion transport. When mitochondrial function is impaired and ATP production is insufficient, muscles lose the energetic capacity to complete this cycle efficiently. This is one of the reasons why metabolic health and mitochondrial function are not peripheral considerations in chronic muscle pain — they are central to whether the tissue can physiologically relax.
Are centrally and peripherally acting muscle relaxers ever used together?
They can be, and the rationale is that they work at different levels — one addressing the nervous system output driving elevated tone, the other addressing the muscular receptor directly. The clinical picture that requires both is one where the nervous system signal is high enough that peripheral calmodulin blockade alone is insufficient. The limitation remains the same for both: neither resolves the autonomic or inflammatory state driving the pattern, so the benefit is sustained only as long as the medications are continued.



Comments