Why Ketamine and Opioids Stop Working for Chronic Pain (And What That Means for Your Recovery)
- Jason Winkelmann
- Jun 16
- 10 min read


TL;DR
Ketamine and opioids are two of the most powerful tools in pain management, and two of the most misunderstood. Most patients on opioids were never told that long-term use can trigger four separate biological mechanisms that make pain worse, not better. Most patients prescribed ketamine were never told exactly what it is correcting and why the correction is temporary. Understanding the physiology behind both medications (what they do, what they cannot do, and what the body actually needs instead) is not academic. For anyone whose medication has stopped working or started requiring higher and higher doses just to maintain the same effect, it is the most important explanation you have probably never received.
What Most Patients Are Told
Ketamine is for severe cases. Opioids are for serious pain. Both are powerful, both carry risk, and neither comes with a thorough explanation of the mechanism.
Most patients on opioids know they are habit-forming. What they are almost never told is the specific biological reason why the medication that worked so well at the beginning gradually loses its effectiveness. And why, in some patients, it eventually begins actively amplifying the pain it was originally prescribed to treat.
Most patients offered ketamine know it is unconventional. What they are almost never told is exactly which mechanism it is targeting, why that mechanism matters, and what would need to be true in their body for the treatment to produce lasting benefit versus temporary relief.
This is not information that is being withheld out of carelessness. It is information that, in most clinical settings, there simply is not time or framework to convey. But the absence of it leaves chronic pain patients without the understanding they need to make sense of their own experience; including the deeply frustrating experience of a medication that used to help and now does not.
Where The Conventional Explanation Breaks Down
Both ketamine and opioids are working on a system called central sensitization. It is the process by which the central nervous system becomes chronically sensitized to pain, allowing more pain signals through and generating pain from inputs that should not be painful at all.
Central sensitization is not a side effect of chronic pain. It is one of its defining mechanisms. It is why chronic pain is so different from acute pain, why it does not respond predictably to the same tools that work for a broken bone or a surgical recovery, and why medications that target peripheral pain (the pain at the site of injury or inflammation) often fall short.
To understand what these medications are doing and where they stop, you first need to understand how pain signals travel and what keeps them in check under normal conditions.
The Gate That Stops Working
When a pain signal arrives at your spinal cord, it enters a structure called the dorsal horn: a relay station where the incoming nerve meets the next nerve in the chain that will carry the signal to the brain.
At that junction, the first nerve releases excitatory neurotransmitters, primarily glutamate and substance P, into the space between the two nerves. The second nerve absorbs those neurotransmitters through a receptor called the NMDA receptor, and the signal continues upward to the brain where it is processed as pain.

Under healthy conditions, this system has a built-in counterbalance. A class of cells called inhibitory interneurons monitors the junction and releases inhibitory neurotransmitters, particularly GABA, into the space between the nerves, effectively blocking a portion of the excitatory signal from getting through. This is descending inhibition: the nervous system's own volume control for pain.

In chronic pain, this volume control fails. The inhibitory interneurons are underperforming, the NMDA receptor is chronically overactivated, and more glutamate is getting through to the second nerve than should be. Inputs that would normally produce no pain, or mild discomfort, are processed as significant pain because the gate is not doing its job.
This is central sensitization. It is a hallmark of virtually every chronic pain condition.
Both ketamine and opioids work on this system. What distinguishes them is where they intervene and what the intervention costs.
Ketamine: Blocking the Receptor That Central Sensitization Depends On
What Ketamine Actually Does
Ketamine works by blocking the NMDA receptor, which is the receptor on the second nerve that absorbs glutamate and other excitatory neurotransmitters from the first nerve.

When the NMDA receptor is blocked, glutamate cannot cross the junction. The excitatory signal cannot reach the second nerve. The volume of pain transmission drops, often dramatically. For patients with severe central sensitization — where the NMDA receptor is chronically overactivated and the inhibitory interneurons are not compensating — this can produce significant and rapid relief where almost nothing else has worked.
This is why ketamine is typically reserved for the most severe chronic pain conditions, including complex regional pain syndrome. It is targeting the specific receptor that central sensitization depends on, and blocking it forcefully.
Where the Mechanism Has Limits
There are two important constraints on ketamine's effectiveness.
The first is mechanistic. Ketamine works specifically on central sensitization driven by NMDA receptor overactivation combined with inadequate descending inhibition. If your chronic pain is being driven by other mechanisms — peripheral inflammation, structural dysfunction, emotional dysregulation, hormonal imbalance — ketamine addresses none of them. The overlap between the mechanism and your specific situation determines whether the treatment produces meaningful benefit.
The second is pharmacological. Ketamine is a dissociative anesthetic. Its side effects (out-of-body experiences, sedation, nausea, perceptual distortion) are direct consequences of how it interacts with the nervous system. These are not rare or idiosyncratic reactions. They are what ketamine does. For most chronic pain patients, these effects make it unsuitable as an ongoing treatment, which is why its use is typically reserved for severe cases where other options have been exhausted.
The Natural Alternative: Support What Ketamine Is Compensating For
Ketamine is blocking the NMDA receptor because central sensitization has driven it into a chronically overactivated state and the inhibitory interneurons are no longer providing adequate counterbalance. The more sustainable target is correcting both of those underlying problems rather than pharmacologically overriding them.
Magnesium blocks the NMDA receptor through the same mechanism as ketamine, though considerably less potent. It will not produce the dramatic acute relief of an infusion. But as part of a broader approach that is also addressing descending inhibition and the conditions driving NMDA overactivation, it is a meaningful and well-supported tool.
Rebuilding descending inhibition requires improving the body's production of the neurotransmitters the inhibitory interneurons depend on, like serotonin, norepinephrine, and GABA. These have been covered in detail in previous posts in this series. The short version is that these are not mysterious compounds. They are synthesized from specific amino acids using specific cofactors, and when those raw materials and cofactors are present in adequate supply, production increases. Addressing gut health, nutritional status, autonomic nervous system balance, and sleep quality are all inputs to this system.
Opioids: A Mechanism the Body Was Already Using — And What Happens When It Gets Overwhelmed
Before anything else, a clarification that matters.
This is not an anti-opioid position. This is a pro-physiology position. Understanding how opioids work, including what goes wrong with long-term use, is not a reason to dismiss them. It is the information you need to understand your own experience and to have a more complete conversation with your provider about what your treatment should actually look like.
The Mechanism That Makes Them Work
Opioid receptors are distributed throughout the nervous system. They are on the first nerve before the junction, on the second nerve receiving the signal, and on the inhibitory interneurons between them.
When an opioid binds to the receptor on the first nerve, it reduces how much glutamate and substance P that nerve releases into the junction. When it binds to the second nerve, it reduces how much the nerve absorbs. And when it binds to the inhibitory interneurons, it activates them; boosting descending inhibition and closing the gate.

This is essentially what your body's own endogenous opioids, endorphins, enkephalins, are already doing. Synthetic opioids work through the same receptors, just much more forcefully. For acute pain, this mechanism is appropriate and effective. The problem, documented clearly in the research and almost never adequately explained to patients, is what happens when that mechanism operates long-term.
The Four Ways Long-Term Opioid Use Can Make Pain Worse
This is the part most patients are never told. It has a name: opioid-induced hyperalgesia — a paradoxical effect in which the medication designed to reduce pain begins making the patient more sensitive to it. It is not a sign of addiction, and it is not a character flaw. It is the predictable physiological consequence of four distinct mechanisms.
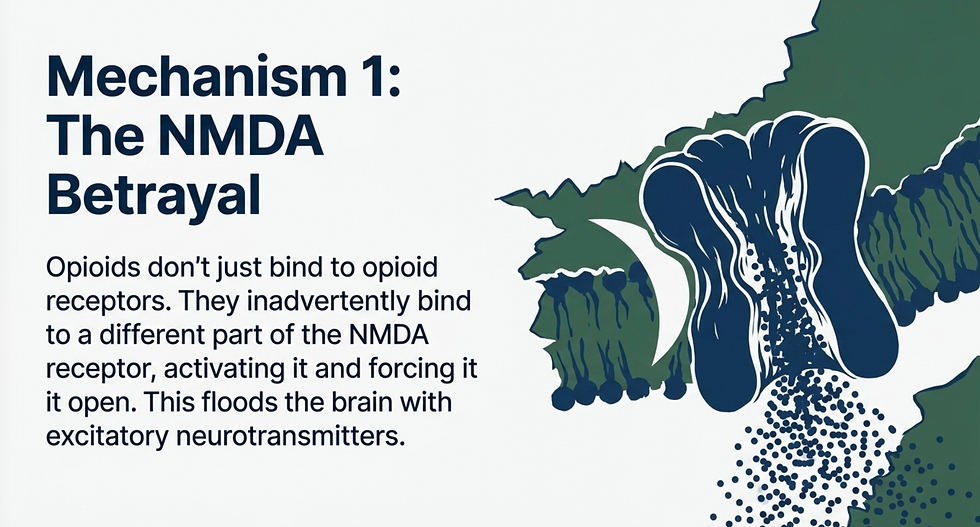
First: NMDA receptor activation. Opioid receptors are not the only receptors on your nerve cells. The NMDA receptor is there as well. Opioids bind to a different site on the NMDA receptor than ketamine does, and rather than closing it, they activate and open it. This is the opposite of what ketamine produces. Over time, more glutamate gets through to the second nerve, not less. The very pathway opioids were suppressing through the opioid receptor is being reopened through the NMDA receptor.
Second: receptor reconfiguration. Under normal conditions, opioid receptors are in what is called a Gi-coupled configuration making them inhibitory in nature. With chronic opioid use, this configuration converts to a Gs-coupled configuration, which makes the receptor excitatory. The receptor that was blocking pain signals begins generating them. The pharmacology of the medication has not changed. The biology of the receptor has.

Third: microglial activation. Microglia are the primary immune cells of the brain and spinal cord. Chronic opioid use activates them, and activated microglia release pro-inflammatory cytokines, generating neuroinflammation. Neuroinflammation increases the excitability of pain-processing neurons and is one of the central drivers of central sensitization. The medication prescribed for chronic pain is worsening one of chronic pain's most important underlying mechanisms.

Fourth: hormonal disruption. Chronic opioid use suppresses the production of testosterone and estrogen. Beyond their other roles in chronic pain, estrogen is required for the synthesis of serotonin. Less estrogen means less serotonin. Less serotonin means the inhibitory interneurons responsible for descending inhibition have less of the neurotransmitter they depend on to do their job. The gate weakens further.

This is the biological explanation for an experience that is both extremely common and almost never adequately explained: opioids worked well initially, then gradually required higher doses to produce the same effect, and eventually the pain became worse despite continued use. This is not tolerance in the conventional sense. It is the nervous system being progressively reconfigured by the medication itself.
The Natural Alternatives: Reduce Reliance, Improve Response
The goal here is not to suggest that these medications should simply be discontinued. It is to identify what the biology actually needs so that any pharmacological intervention can be more effective, safer, and supported by a system that is working rather than one that is compensating for its own depletion.
Increase endogenous opioid production. Your body produces its own opioids in the form of endorphins and enkephalins, and there are well-studied ways to increase their production. Movement and exercise are the most direct and evidence-supported inputs. Chiropractic care and acupuncture have documented effects on endogenous opioid release. Strong social connections, laughter, music, and dance all produce measurable increases in endorphin activity. These are not offered as replacements for severe pain management. They are offered as genuine contributors to a system that, when functioning better, reduces reliance on synthetic inputs.
Improve NMDA receptor sensitivity with magnesium, addressing one of the four mechanisms by which chronic opioid use amplifies pain.
Rebuild descending inhibition by supporting serotonin, norepinephrine, and GABA production, which directly counteracts the hormonal and neurotransmitter depletion that opioids produce over time.
Reduce neuroinflammation through gut health, nutritional support, and the interventions that address microglial activation. Activated microglia are not just a consequence of opioid use; they are also driven by gut permeability, blood sugar dysregulation, and chronic stress, all of which can be meaningfully addressed.
The Pattern That Runs Through Both
Ketamine blocks the NMDA receptor that central sensitization has driven into overdrive without restoring the descending inhibition that failed to prevent the overdrive in the first place.
Opioids suppress pain transmission through receptors the nervous system was already using, without addressing what made the nervous system unable to manage pain on its own. And in the process, trigger biological changes that progressively undermine the treatment.
In both cases, the medication is a powerful intervention on a system that is already failing. What neither medication does is address why the system is failing, and that is why, in chronic pain, both eventually stop being sufficient on their own.
The Bottom Line
If your medication worked at first and works less well now, that is not a coincidence. It is a mechanism.
And a mechanism that can be understood can, in most cases, be addressed.
The path forward is not a stronger drug. It is understanding what your biology needs and building a treatment plan that actually provides it.

Written By:
Dr. Jason Winkelmann
Naturopathic doctor, Chiropractor, Chronic Pain Specialist, and Educator
Frequently Asked Questions
I've been on opioids for years and my pain is worse than when I started. Is that actually the medication?
It can be — and it is more common than most patients are told. Opioid-induced hyperalgesia is a well-documented physiological phenomenon in which long-term opioid use triggers changes to the NMDA receptor, the configuration of opioid receptors themselves, microglial activation, and hormonal disruption that collectively increase pain sensitivity over time. This does not happen identically in every patient, and it does not mean the medication was the wrong choice at the beginning. It means the biology of long-term opioid use is more complex than the initial mechanism suggests, and that complexity needs to be part of the clinical conversation.
Why does ketamine work for some people and not others?
Ketamine specifically targets NMDA receptor overactivation combined with inadequate descending inhibition. If your chronic pain fits that profile — if central sensitization driven by glutamate excess and failing inhibitory interneurons is a central mechanism — ketamine can produce significant relief. If your pain is being driven primarily by other pathways, the NMDA receptor is not the limiting factor and blocking it will not change much. This is not a failure of the treatment in isolation. It is a mismatch between the mechanism of the drug and the mechanism of the condition.
My doctor mentioned opioid tolerance. Is that the same as opioid-induced hyperalgesia?
They are related but distinct. Tolerance refers to the receptor becoming less responsive to the drug over time, requiring higher doses to produce the same effect. Opioid-induced hyperalgesia is different — it is an active increase in pain sensitivity caused by the four biological mechanisms described above. The practical experience can look similar: more medication producing less relief, with the pain eventually exceeding pre-treatment levels. But the underlying mechanism and the appropriate clinical response are different, which is why this distinction matters for your care.
Can the biological changes from long-term opioid use be reversed?
Many of them can be improved, though the degree and timeline depend on how long the medications were used, the doses involved, and the state of the underlying systems. NMDA receptor sensitivity can be supported with magnesium. Descending inhibition can be rebuilt by addressing neurotransmitter production. Microglial activation can be reduced through interventions that lower neuroinflammation. Hormonal disruption requires its own evaluation and support. None of this happens quickly, and none of it is best managed without clinical guidance — but the mechanisms are addressable, and improvement is genuinely achievable in most patients who address them systematically.
Is there a natural equivalent to ketamine?
Not in terms of potency or speed of effect. Ketamine produces rapid, forceful NMDA receptor blockade that no natural intervention replicates at that level. Magnesium operates through the same mechanism but considerably more gently. What natural approaches can do — and what they are genuinely capable of when applied comprehensively — is address the underlying conditions that drove the NMDA receptor into an overactivated state in the first place: neuroinflammation, neurotransmitter depletion, autonomic dysregulation, and gut permeability. Resolving the inputs that created the problem is more durable than blocking the receptor the problem is expressed through.


Comments