Chronic Pain Medications Explained: How They Work, Their Limitations, and Natural Alternatives
- Jason Winkelmann
- 33 minutes ago
- 13 min read


TL;DR
Antidepressants, anti-anxiety medications, JAK inhibitors, and CGRP blockers are among the most commonly prescribed drugs for chronic pain conditions. But most patients are never given a complete explanation of what they actually do. More importantly, they are almost never told what these medications fail to do, why the side effects happen, and what the underlying biology would need instead. This article covers all four: the mechanism, the gap, the consequences, and the alternatives, so that you can finally understand the full picture of what is and is not happening with your treatment.
What Most Patients Are Told
When a chronic pain patient receives a prescription for an antidepressant or an anti-anxiety medication, the explanation offered is usually incomplete at best. You might be told that these medications help modulate pain signals, or that they address the emotional component of chronic pain, or that they work on the nervous system in ways that reduce sensitivity.
For JAK inhibitors and CGRP blockers, often prescribed for inflammatory conditions and migraines respectively, the explanation tends to focus on what the drug blocks, with far less discussion of what that same block is simultaneously preventing your body from doing.
What is almost universally left out is the physiology behind why the drug works, why it is insufficient on its own, and why specific and predictable problems arise with long-term use.
Understanding that physiology is not semantics. It is the most direct path to understanding why you may still be in pain despite being on medication, and what would actually need to change for that to be different.
Where The Conventional Explanation Breaks Down
The pattern across all four medication categories covered in this article is the same one that runs through every conventional approach to chronic pain management.
Each drug targets a specific mechanism that is contributing to pain and either blocks it, suppresses it, or artificially augments it. Each produces a measurable effect. And each one leaves the conditions that created the problem fully intact. Which is why, in chronic pain, the relief tends to be partial, temporary, or dependent on continued use.
This is not a failure of the medications. They are doing what they were designed to do. It is a failure of the model that treats symptom reduction and condition resolution as the same goal.
Antidepressants: Preserving What You Have When You Need More of It
To understand why antidepressants are prescribed for chronic pain — and why they are not enough, you first need to understand a mechanism called descending inhibition.
The Gating System Nobody Explains
Every nerve in your body fires at the same intensity. There is no dial. When a nerve fires, it fires at 100 percent. This raises an obvious question: why does stubbing your toe feel so much worse than bumping your elbow if the nerves are firing at the same intensity?
The answer is that your spinal cord functions as a gating system, determining how much of any incoming pain signal is allowed to reach your brain to be processed as pain.
When you bump your elbow, your spinal cord essentially determines that the signal is not especially threatening and sends inhibitory signals back down to block most of it so that only a small fraction reaches your brain. When you stub your toe, the gate opens wider, more of the signal gets through, and you feel significantly more pain.

Two neurotransmitters that determine how much descending inhibition your spinal cord produces are serotonin and norepinephrine. More of both means a stronger gate. Less of both means the gate weakens, more pain signals get through, and you begin experiencing pain more intensely than the input justifies.
This weakening of the gate is called central sensitization, and it is the defining feature of virtually every chronic pain condition.

What Antidepressants Actually Do
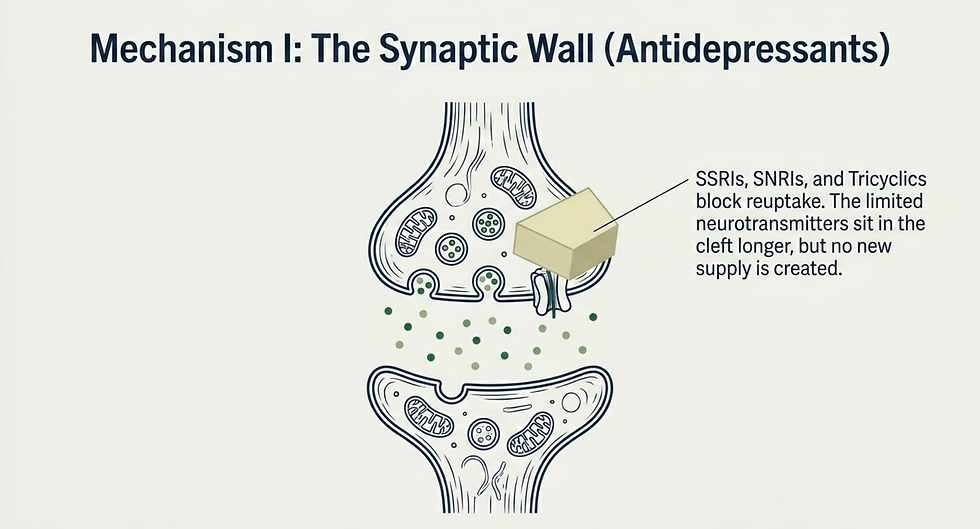
SSRIs, SNRIs, and tricyclic antidepressants all work by preventing the reuptake of serotonin and norepinephrine at the nerve synapse.
Here is how that works. Your nervous system is not just one continuous nerve from brain to specific body part. There are multiple nerves along this pathway and they work together to get the job done. The first nerve releases serotonin and norepinephrine into the gap between itself and the next nerve. The second nerve takes in those neurotransmitters and the signal continues on to the next nerve. Whatever neurotransmitters the second nerve does not immediately take in, the first nerve takes back for recycling. The longer those neurotransmitters sit in the gap, the more the second nerve can take in, which intensifies the pain-blocking signal.
These medications block the reuptake process, allowing the serotonin and norepinephrine to sit in the gap longer and giving the next nerve a better chance of taking them up.
SNRIs and tricyclics tend to be more effective for chronic pain than SSRIs specifically because they preserve both serotonin and norepinephrine. Both of the neurotransmitters involved in descending inhibition. Rather than serotonin alone.
It is a rational mechanism, but it has a significant limitation.
Why Preserving Is Not The Same As Producing
If the underlying problem is that your body is not making enough serotonin and norepinephrine to begin with, then preserving what little exists produces only a marginal improvement. You are extending the lifespan of a depleted supply rather than restoring it.
This is precisely why antidepressants produce partial and inconsistent results in chronic pain, and why some patients experience meaningful benefit while others see almost none.
The difference often comes down to how depleted their baseline neurotransmitter production was before the medication was started.
The Natural Alternative: Build the Supply
The more productive treatment is to help the body produce more serotonin and norepinephrine, not just recycling what it has.
Serotonin is synthesized from an amino acid called tryptophan. The conversion requires a specific set of cofactors: iron, magnesium, calcium, vitamins B6, B9, and C, and zinc. Without adequate levels of these, the biochemical pathway stalls regardless of how much tryptophan is available.

It is important to note that serotonin is necessary to make melatonin. If you are living with chronic pain and also struggling with sleep disturbances (and most people are) this connection is meaningful. Supporting serotonin production does not just strengthen descending inhibition. It supports sleep quality as well, which is one of the primary windows during which the body clears inflammatory waste and repairs tissue.
Norepinephrine is synthesized from a different amino acid called tyrosine, with iron, B6, and vitamin C as key cofactors. Critically, dopamine is produced as an intermediate step in this pathway. Dopamine is not only your primary reward and motivation neurotransmitter, it also contributes independently to descending inhibition. Supporting norepinephrine synthesis means supporting dopamine production as well.
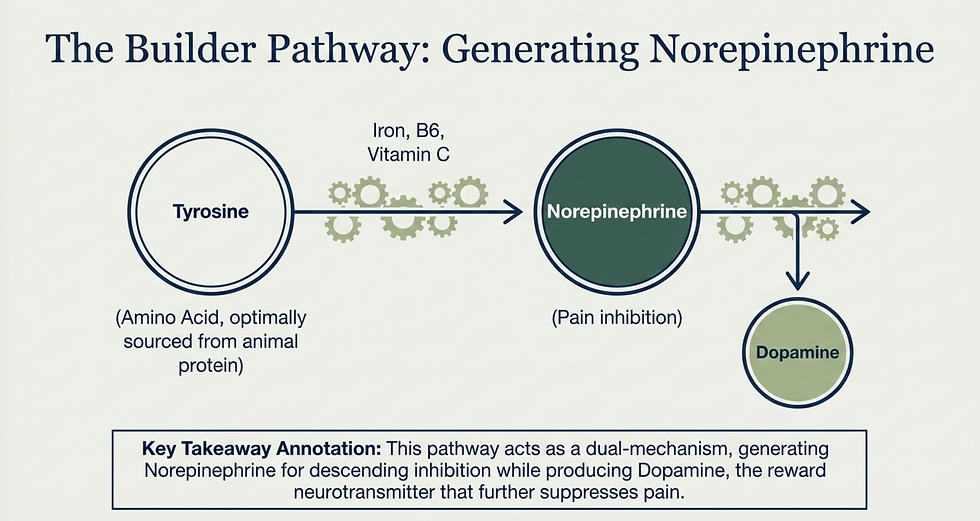
The most accessible way to support both pathways simultaneously is simply increasing dietary protein intake, particularly from animal sources that provide a complete and bioavailable amino acid profile. Supplementing individual cofactors can be useful on top of that, particularly when specific deficiencies are identified.
Anxiolytics: Managing the Alarm Without Resolving What Triggered It
How Fear and Anxiety Generate Physical Pain
When your brain perceives a threat — physical or emotional, real or anticipated — it activates the amygdala, one of the brain's primary threat-detection centers and one of 44 regions associated with chronic pain processing.
That amygdala activation drives sympathetic nervous system dominance, which increases muscle tension and lowers your threshold for pain perception. You become more vigilant, more reactive, and more sensitive. Which is adaptive in genuine danger, but deeply counterproductive as a chronic state.
The inhibitory neurotransmitter GABA acts as a counterbalance to this. When GABA is present in adequate amounts at the right places, it suppresses the excitatory signaling that keeps the nervous system in a heightened state. It strengthens descending inhibition and helps regulate the sympathetic-parasympathetic balance.

Benzodiazepines (the primary class of anxiolytic medications) work by enhancing GABA's effect at its receptor. The result is a calmer nervous system, reduced muscle tension, and a meaningful reduction in pain sensitivity for many patients.
The Same Problem Restated
Think of the pain pathway as a conflict between two forces: one trying to send the pain signal through and one trying to suppress it. GABA is on the suppression side. More GABA means more inhibitory troops and a stronger chance of winning the conflict before the pain signal reaches the brain.
Benzodiazepines amplify whatever GABA is present. But if GABA production is chronically low — which it often is in people living with chronic stress, gut dysfunction, and nutritional deficiencies — you are amplifying a small force rather than building a larger one.
Long-term benzodiazepine use also carries well-documented consequences: physical dependence, cognitive blunting, impaired memory, and a rebound effect when the medication is reduced or discontinued. The nervous system adapts to the artificial GABA amplification by downregulating its own GABA receptors, meaning the patient ends up with less functional GABA signaling than they started with once the drug is removed.
The Natural Alternative: Produce More GABA
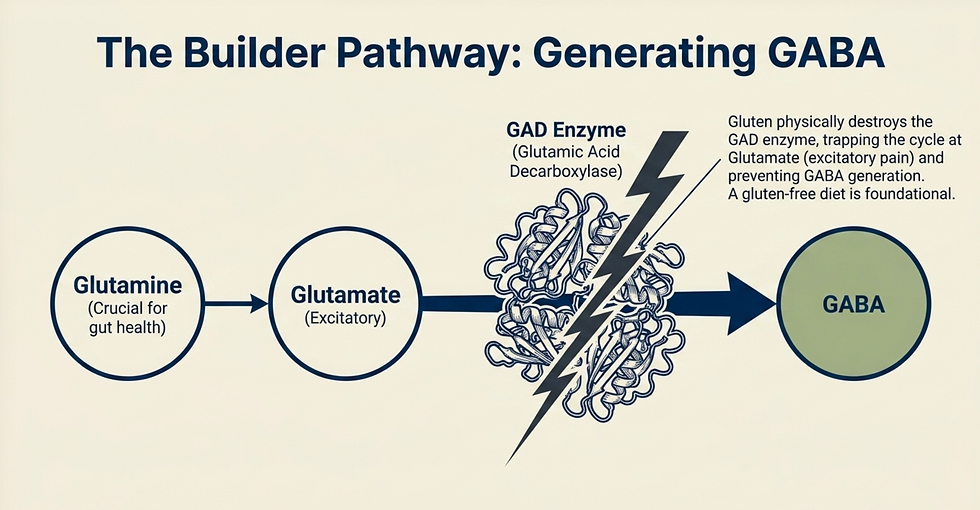
The body synthesizes GABA from glutamate through an enzyme called glutamic acid decarboxylase. Here is a detail that is almost never explained in a clinical context: this enzyme is directly inhibited by gluten.
This is one of the most physiologically concrete explanations for why a gluten-free diet produces neurological and pain-related benefits that go well beyond gastrointestinal symptoms. It is not about gut sensitivity alone. When gluten is consistently present, the enzyme that converts glutamate into GABA is suppressed. This means more glutamate (an excitatory neurotransmitter) remains, and less GABA (the inhibitory counterbalance) is produced.
The starting material for this pathway is glutamine, an amino acid that is also one of the primary fuels for the cells lining your gut wall. Supporting glutamine intake addresses both gut integrity and GABA production — two of the most critical targets in chronic pain — simultaneously.
Additional support for GABA synthesis comes from vitamin B6, which acts as a cofactor in the conversion process. Fermented foods and high-quality probiotics contribute as well, since a substantial portion of GABA is actually synthesized by the gut microbiome. Another reason gut health sits at the center of every meaningful chronic pain treatment approach.
In addition to increasing GABA production, we need to balance the autonomic nervous system; and this takes more than supplementation. Consistent movement, breathwork, yoga, and meditation all produce measurable increases in GABAergic activity through neuroendocrine pathways. These are not suggested because they are easy or convenient. They are suggested because the research behind them is consistent and the mechanism is well understood.
JAK Inhibitors: Blocking the Whole Switch to Turn Off Half of It
The JAK-STAT Pathway
When a cytokine (a type if chemical messenger) binds to a receptor on your cell membrane, it activates a family of enzymes called Janus kinases, or JAK. Activated JAK enzymes attach a phosphate group to a protein called STAT, which then travels to the cell nucleus and acts as a switch — turning on genes that either promote or resolve inflammation, depending on which cytokine initiated the cascade.
JAK inhibitors, sometimes called JAK-STAT inhibitors, work by placing a block between JAK and STAT, preventing the STAT protein from receiving the signal that would otherwise send it to the nucleus.

The intended effect is that pro-inflammatory genes do not get turned on. And in conditions driven by autoimmune cytokine activity — rheumatoid arthritis, psoriatic arthritis, certain inflammatory bowel conditions — the reduction in inflammatory signaling can be significant.
Why This Mechanism Creates the Problems It Does
The problem is structural. The JAK-STAT switch does not distinguish between pro-inflammatory and anti-inflammatory signals. When the pathway is blocked, neither type of gene is being activated.
This means that while pro-inflammatory gene expression is being suppressed, so is the body's ability to turn on anti-inflammatory genes. Inflammation that has already been produced has fewer mechanisms for resolution. And because the upstream cytokine production has not been addressed (JAK inhibitors do not affect what triggers cytokine release in the first place) the pro-inflammatory cytokines continue to form and continue generating inflammation through mechanisms that do not depend on the JAK-STAT pathway.
The immune suppression that results is not a side effect in the conventional sense. It is a direct consequence of blocking a pathway that immune function depends on. Increased susceptibility to infection, elevated risk of cardiovascular events including heart attack and blood clot, and a modestly increased risk of certain cancers including lymphoma and non-melanoma skin cancers are all the predictable downstream result of sustained JAK-STAT suppression.
The Natural Alternative: Treat the Epigenetics
The more fundamental target is the upstream regulation of which genes are being turned on in the first place. That is an epigenetic question, one that is largely addressed through the environment the body is living in.
Gut permeability drives chronic immune activation by allowing particles into circulation that should not be there, triggering persistent cytokine production. Unresolved chronic infection creates ongoing inflammatory signaling. Blood sugar dysregulation activates the same nuclear factor kappa-beta pathway that drives systemic inflammation. Sleep deprivation impairs the body's ability to resolve inflammation during the critical overnight window. Environmental triggers — from food sensitivities to chemical exposures — maintain a state of low-grade immune activation that keeps the system running hot.
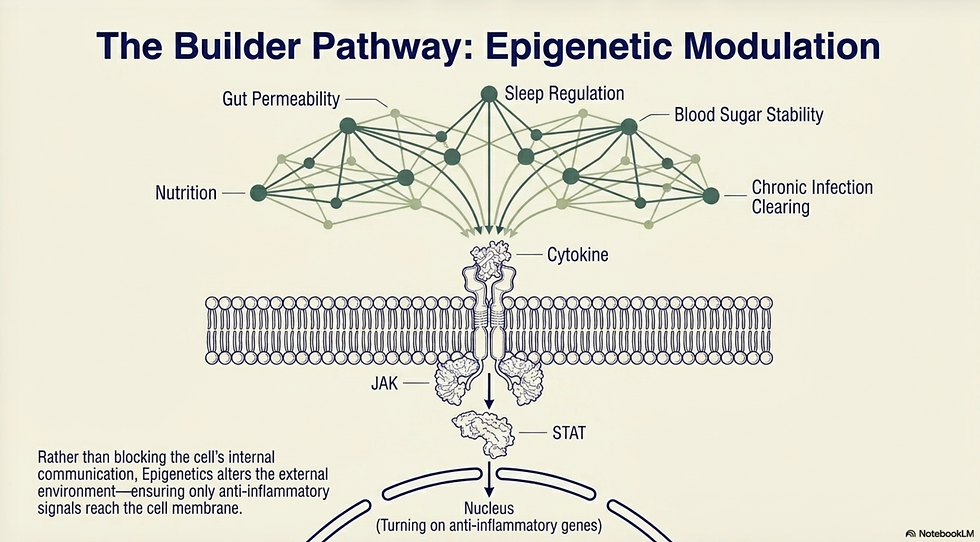
Treating the epigenetic inputs that determine gene expression does not produce the fast, dramatic symptom relief of a JAK inhibitor. But it changes what genes are being switched on, rather than blocking the switch entirely and eliminating the body's ability to regulate its own inflammatory response.
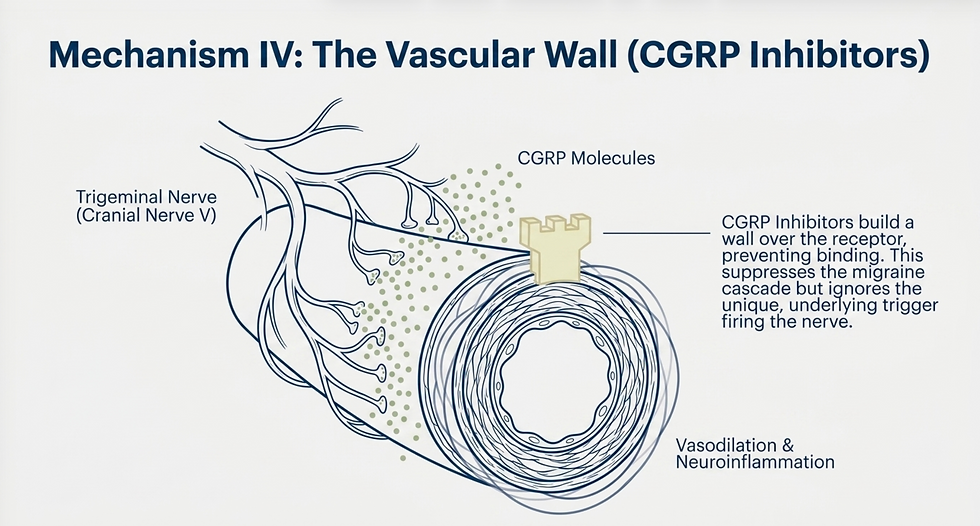
CGRP Inhibitors: One Mechanism in a Multi-Mechanism Condition
The Migraine Cascade
Migraines are not headaches. They are neuroinflammatory events, and treating them only at the point of pain is one of the primary reasons migraine management produces such inconsistent results.
The cascade typically begins with a personal trigger: a food sensitivity, hormonal fluctuation, environmental exposure, or stress response. That trigger activates the trigeminal nerve, the fifth cranial nerve that wraps around the face and head. Once activated, the trigeminal nerve releases inflammatory molecules, primarily a peptide called calcitonin gene-related peptide, or CGRP.
CGRP binds to receptors on blood vessels and causes them to dilate. That vasodilation brings a flood of pro-inflammatory cytokines to the brain tissue, driving neuroinflammation. Both generate pain and increase future sensitivity, making subsequent triggers more likely to cross the threshold that sets off the cascade.
CGRP inhibitors block both the release of CGRP and its binding to vascular receptors, preventing the dilation and the subsequent inflammatory cascade from occurring.
For patients whose migraines are being primarily driven by excessive CGRP release, these medications can meaningfully reduce frequency and intensity. That is a real benefit.
What the Medication Leaves Intact
CGRP is one mechanism in a condition that involves multiple converging pathways. The trigger that activated the trigeminal nerve in the first place has not been identified or addressed. The systems that would ordinarily handle that trigger without generating a full migraine cascade — gut function, hormonal regulation, nervous system stability, inflammatory threshold — have not been evaluated or treated.
This is why CGRP inhibitors work well for some patients and produce limited benefit for others. The ones who respond well are those whose migraines happen to be predominantly CGRP-driven. Those who do not respond are those whose cascade is being initiated or sustained through other pathways that the medication does not touch.
Natural CGRP Inhibitors and the More Important Target
Several natural compounds have documented CGRP-inhibiting activity: CoQ10, the herb butterbur, magnesium, and curcumin. They are not as pharmacologically potent as CGRP inhibitor medications, but as part of a comprehensive treatment approach, they can contribute meaningfully to reducing migraine frequency and intensity.

More importantly, the primary target for migraine treatment is not CGRP. It is the stabilization of the systems that determine whether a given trigger generates a migraine at all. The goal is not to block the cascade mid-stream. It is to reduce the nervous system's reactivity and the inflammatory threshold to the point where ordinary triggers are handled without triggering the full cascade.
That means addressing gut health if food sensitivities are contributing. It means regulating blood sugar and hormonal patterns that are known to precede migraine onset. It means treating the autonomic dysregulation that keeps the trigeminal system sensitized. CGRP inhibitors do none of those things. And for the patient whose migraines have not resolved on them, this is almost certainly the reason why.
What All Four Medications Share
Antidepressants preserve neurotransmitters without building them. Anxiolytics amplify GABA without producing it. JAK inhibitors block the inflammatory switch without addressing what is triggering the signal. CGRP inhibitors interrupt one pathway in a multi-pathway condition without stabilizing the systems that determine whether that pathway gets activated.
In each case, the mechanism being targeted is real, and the physiological rationale is sound. But in each case, the underlying biology that created the problem continues operating, unaddressed, while the medication manages the downstream consequences.
This is not a reason to avoid medication. It is a reason to understand that medication alone is not a treatment plan. In a comprehensive approach, some of these drugs have legitimate supporting roles. As the primary or only intervention, they leave the most important work undone.
The Bottom Line
If you are taking one or more of these medications and you are still suffering, it is not because you have not given them enough time or not taken them correctly.
It is because the conditions producing your pain have not been treated, and no amount of signal management changes that.
The question was never whether your medications work. The question is whether they are addressing what is actually wrong.

Written By:
Dr. Jason Winkelmann
Naturopathic doctor, Chiropractor, Chronic Pain Specialist, and Educator
Frequently Asked Questions
My antidepressant was prescribed specifically for pain, not depression. Does it still work the same way?
Yes. When antidepressants are prescribed for chronic pain, the target is the descending inhibition pathway in the spinal cord, not the mood-regulating pathways in the brain. The mechanism — preserving serotonin and norepinephrine at the synapse — is the same regardless of why the medication was prescribed. The limitation is also the same: if baseline neurotransmitter production is insufficient, there is a ceiling to how much preservation can accomplish.
Why do benzodiazepines cause dependence when they are just increasing GABA?
Because the nervous system adapts to the artificial amplification. When GABA receptors are consistently being over-stimulated by the medication, the brain compensates by reducing the number or sensitivity of those receptors. Over time, normal GABA levels are no longer sufficient to produce adequate inhibition — meaning the patient requires the medication to achieve a baseline state that their nervous system used to be able to maintain on its own.
JAK inhibitors are prescribed for serious autoimmune conditions. Are the risks really that significant?
The risks are real and they are printed in the prescribing information. For patients with severe autoimmune disease that has not responded to other treatments, the benefit-risk calculation may be appropriate. The point is not that these medications should never be used — it is that the side effects, including immune suppression, cardiovascular risk, and cancer risk, are the direct consequence of how the medication works, not incidental effects. Understanding that should inform how aggressively the underlying drivers are being addressed alongside the medication.
If natural CGRP inhibitors are less potent than the medication, why use them at all?
Because in a comprehensive treatment approach, they do not need to carry the full load. When gut health, blood sugar regulation, hormonal balance, and autonomic nervous system function are being addressed simultaneously, the threshold for triggering the migraine cascade rises. Natural compounds that modestly reduce CGRP activity, combined with a system that is less reactive to begin with, can produce outcomes that either medication or lifestyle changes alone cannot. The goal is a stable system, not just a blocked pathway.
Why does gluten specifically block GABA production?
Gluten contains peptides that inhibit glutamic acid decarboxylase, the enzyme that converts glutamate into GABA. This is a well-documented mechanism in the research literature on non-celiac gluten sensitivity and its neurological effects. It does not require celiac disease or a diagnosed gluten sensitivity to occur — the enzyme inhibition happens in the presence of gluten regardless of whether GI symptoms are present. This is one of the most important and least communicated reasons why a gluten-free dietary approach produces benefits across multiple chronic pain conditions.


Comments